10 Dec 2012
This article is part of the network’s archive of useful research information. This article is closed to new comments due to inactivity. We welcome new content which can be done by submitting an article for review or take part in discussions in an open topic or submit a blog post to take your discussions online.
In light of the recent WHO update on the Novel Coronavirus (30 November http://www.who.int/csr/disease/coronavirus_infections/update_20121130/en/index.html), and given the paucity of evidence on which to base treatment and understand disease pathogenesis, ISARIC – a recently formed global clinical research consortium – would like to propose a collaborative clinical research platform. The proposed studies aim to assess prospectively the pathogenesis of illness and potential therapeutic interventions for patients infected with the novel coronavirus (nCoV). Standardized collection of data will facilitate sharing of information among those caring for such patients. The proposals from ISARIC would be open and available to any organization interested in participating.
Though the total number of laboratory confirmed cases to date is low, it is impossible to know how many cases may occur. In addition the patients may be admitted in future to multiple hospitals in many different countries. It is crucial to plan for standardized, prospective data collection in order to understand how to improve the clinical outcome for patients with nCoV. The following suggestions also cover specific therapeutic interventions, which we believe need to be evaluated. These interventions do not include studies on supportive care such as access to critical care, fluid management and organ support as established guidelines, including those of WHO, are available for these.
ISARIC proposed studies
Observational studies should be conducted in the situation of a novel disease, which may occur in a variety of resource settings, and may be the only pragmatic option for data collection available. Clinicians should include data collection on all therapeutic interventions delivered.
Prospective, sequential, standardized clinical data collection and daily sampling for virological and pathogenesis studies should be undertaken, whenever feasible, and with strict adherence to appropriate infection control measures. Where possible we recommend that these clinical saples should be stored, with consent, for future research.
In the absence of evidence to guide treatment we would suggest interventions are delivered as part of a randomized clinical trial (see below). However, we recognize that this may not be possible.
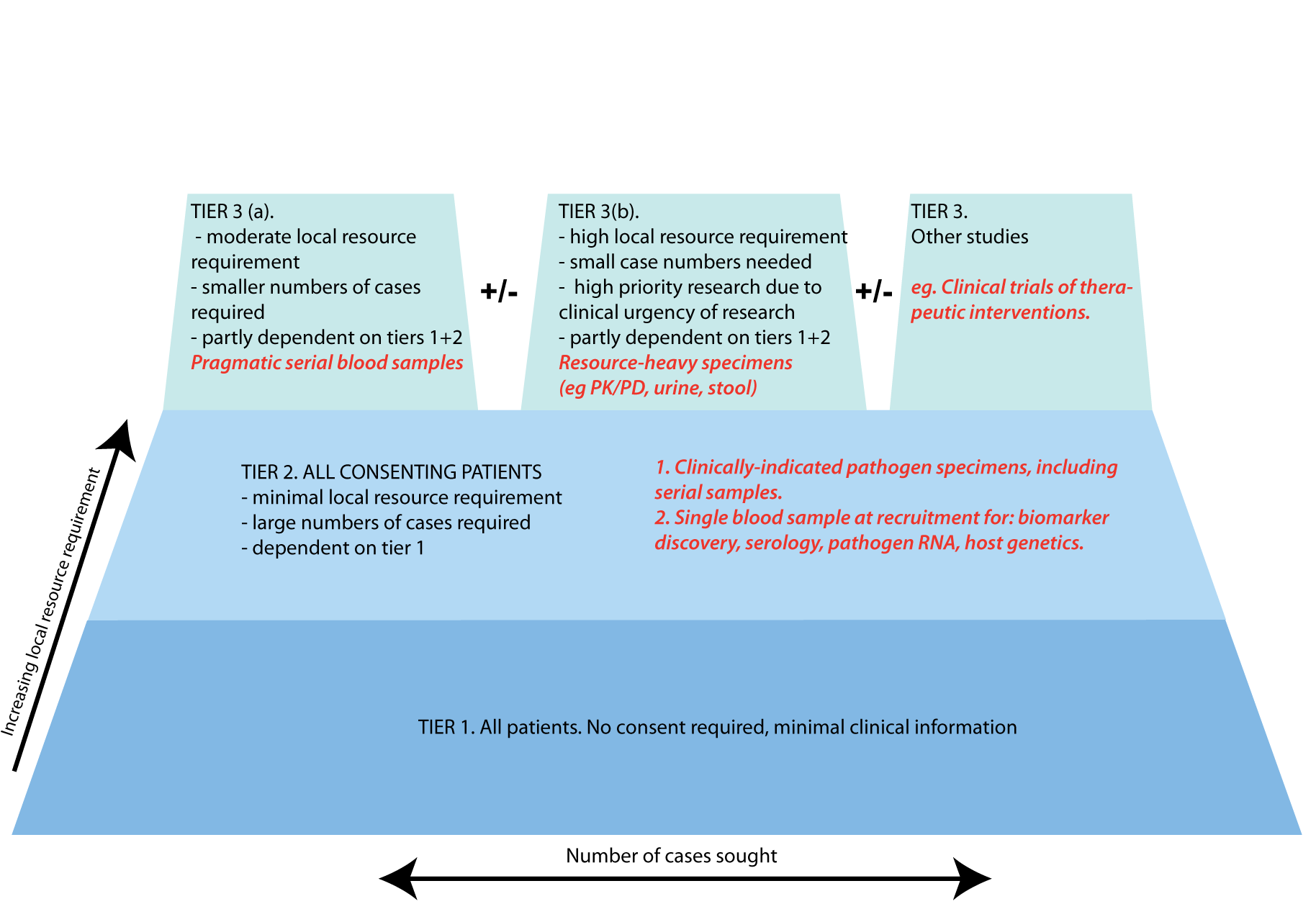
We propose a pragmatic framework in which research protocols developed in different parts of the world may produce results suitable for future collaborative analysis (see full table and diagram: http://isaric.tghn.org/articles/novel-coronavirus-sampling-plan/). In producing this proposal, we assign the highest priority to research questions that will provide information that is immediately clinically relevant. Local resource requirement to recruit cases is the primary determinant of which hospitals can participate. In practice this is the key determinant of the global spread of a research project, and hence the number of cases that can be recruited. We therefore used the local resource requirement to stratify studies: studies on the lowest tier (tier 1, Tiered Strategy: http://isaric.tghn.org/articles/novel-coronavirus-sampling-plan/) may be carried out in almost any hospital that is capable of participating in research, whereas some studies in tier 3 require extensive dedicated research staff in any recruiting centre.
Tiers 1+2 comprise samples and data for studies that both require large numbers of cases but have relatively limited local resource implications. Full recruitment to these studies would require:
1. Consent
2. Storage of all clinically-indicated pathogen samples
3. A single EDTA blood sample at the time of recruitment, to be split into plasma and cell fractions locally.
Tier 3 lists additional studies, all of which are to some extent dependent on Tiers 1+2. A more detailed list of samples proposed in this tier is available for download on ISARIC’s website: http://isaric.tghn.org/articles/novel-coronavirus-sampling-plan/).
Randomized Controlled Trials (RCTs) could be initiated either if sufficient patients are seen at one location or via a collaborative regional or global effort with appropriate ethical approvals in place. Therefore, we suggest that clinicians and researchers consider, in advance, which intervention(s) they would with to evaluate in an RCT and have pre-emptive discussions with ethics committees to expedite decision-making.
Please see the discussion below with our suggestions regarding the therapeutic interventions that could be studied.
We will make available online at www.isaric.org a draft consent form, case report form and outline protocol (adaptable) for anyone either interested in participating in such a collaborative effort or requiring access to these materials for their own use in individual studies.
Potential therapeutic interventions
No antivirals or therapeutics of proven value currently exist for the novel CoV, and insufficient data were generated in studies of patients with the SARS-CoV to be able to guide treatment decisions (Wong and Yuen, J Antimicrob Chem 2008, 62:437; Stockman et al., PLoS Med 2006, 3(9): e343). However, a potential role for antiviral therapy is supported by the observation that viral load is positively correlated with the development of organ dysfunction and death in SARS-CoV patients (Hung IF et al. Emerg Infect Dis 2004, 10:1550). Based on rhesus macaque model and/or clinical studies in SARS, antiviral agents of particular interest would include Interferon-alfa (Loutfy et al., JAMA 2003, 290:3222), neutralizing antibody (convalescent plasma or monoclonal antibodies if/when available) (Yeh et al., JAC 2005, 56:919), and perhaps siRNAs (Li et al., Nature Med 2005, 11:944). Neither systemic ribavirin nor HIV protease inhibitors (lopinavir-ritonavir) were proven beneficial in SARS, and ribavirin was associated with significant side effects. However, the use of lopinavir/ritonavir plus ribavirin was associated with a lower incidence of adverse outcomes including acute respiratory distress syndrome, other adverse outcomes and death and antiviral effects when compared with historical controls who had received ribavirin alone (Chu CM et al., Thorax 2004, 59:252), so that further study appears warranted. Unlike SARS CoV, the nCov does not appear to share the ACE2 receptor (R Fouchier, personal communication), so that inhibitors directed to it are unlikely to be effective. The finding that mannose-binding lectin (MBL) levels were lower in SARS patients (Ip et al., JID 2005, 191:1697) and that MBL can inhibit the SARS-CoV in vitro (Zhou et al., J Virol 2010, 84(17):8753), raise the possibility of using recombinant human MBL, shown active in an Ebola murine model (Michelow et al., JID 2011, 203:175), for treatment.
The role of immunomodulatory interventions in SARS treatment remains unclear. Systemic corticosteroids were commonly used in SARS patients and, while some reports suggested transient effects on fever and pulmonary manifestations, no survival benefit was established and serious adverse effects include increased risk of secondary infections and aseptic necrosis of the hip. The use of corticosteroids was also associated with an increase in the plasma viral load (Lee N et al., J Clin Virol 2004, 31: 304–9). IVIg was not systematically studied in SARS but may warrant further study for both its immunomodulatory effects and possible nCoV inhibitory activity. There is continued interest in the role of statins and other immunomodulatory agents in severe acute respiratory infections in general and these could be considered as part of detailed observational studies or ideally an RCT.
About ISARIC
The International Severe Acute Respiratory and Emerging Infection Consortium (ISARIC) is a global consortium of clinical research networks aiming to change the approach to collaborative patient orientated research between and during rapidly emerging public health threats. A new approach will enable the generation and sharing of new knowledge, complement public health responses, maximize the availability of clinical information and thereby save lives. Being a partner of ISARIC is open to anyone interested in clinical research in rapidly emerging public health threats globally.
We hope that ISARIC, supported by, the Wellcome Trust, Medical Research Council UK, Bill and Melinda Gates Foundation, INSERM France, Singapore Ministry of Health, and the Li Ka Shing Foundation will help facilitate collaborative patient orientated research to complement the public health response in epidemics and pandemics.
http://www.wellcome.ac.uk/News/Media-office/Press-releases/2011/WTVM053638.htm
www.isaric.org
Signed the ISARIC Executive, through
Derek Angus
University of Pittsburg School of Medicine, USA
Kenneth Baillie
The Roslin Institute, University of Edinburgh, UK
Roberto Bruzzone
HKU-Pasteur Research Pole, University of Hong Kong, Hong Kong SAR
Dean Everett
Malawi-Liverpool-Wellcome Trust Clinical Research Programme & University of Liverpool, Malawi
Jeremy Farrar, Chairman ISARIC
Oxford University Clinical Research Unit Hospital for Tropical Diseases Vietnam
Wellcome Trust Programme Vietnam South East Asian Infectious Disease Clinical Research Network (SEAICRN)
Gail Carson
International Severe Acute Respiratory and Emerging Infection Consortium and University of Oxford UK
Zhancheng Gao
Peking University People’s Hospital, China
Frederick Hayden
Wellcome Trust, London UK and University of Virginia School of Medicine, Charlottesville, Virginia, USA
John Marshall
University of Toronto, CCCTG & InFACT, Canada
Gernot Rohde
Maastricht University, The Netherlands
Kathy Rowan
ICNARC, UK
Steve Webb
University of Western Australia, Australia
Please contact Kajsa-Stina Magnusson, ISARIC project manager with any questions at kajsa-stina.magnusson[at]ndm.ox.ac.uk
As broadcast through ProMED, 8 December 2012
Also By
Kajsa-Stina Magnusson
{kind=link}
Related Articles
-
Institutional maternal and perinatal deaths: a review of 40 low and middle income countries
BY Bailey et al -
Zika virus in asymptomatic blood donors in Martinique
BY Gallian et al. -
Antimicrobial Resistance and Immunisation
BY Authors: Sarah Bunn; Catherine Hall -
Biological Informatics Research Training in Health
BY M. Lesosky, C. Reddy -
The International Stroke Trial database
BY Peter AG Sandercock, Maciej Niewada, Anna Członkowska, the International Stroke Trial Collaborative Group